Jan 16, 2024
There’s a piece of my body missing. That’s a big deal.
You wouldn’t have known this growing up in my family. Circumcision was a laughable topic and only regarded as a joke; never in a serious tone, and certainly never condescended upon. Like if we were having hotdogs for dinner, the crude comments would inevitably come up. My older relatives thought it was very funny for some reason, and I could not understand. My mom might wrinkle her nose and softly say something like “That’s nasty.”
Through gritted teeth, I tried not hearing the words—blocking them out as a chilling cocktail of disgust, horror and disbelief coursed through the back of my head and down my spine, seeking refuge from the words that the Grown Ups were saying. How could they not see that this is wrong?
I was circumcised as an infant in a routine hospital procedure. If they had done the right thing and left me alone when I was a baby, I certainly believe I would be a better version of myself than how I actually ended up. Things like trimming my nails bother me to this day; my best friend who trims and styles my long, golden hair probably doesn’t know why I wince at the metallic sound of her scissors.
When I was young, I had a recurring traumatic dream. It’s like I’m watching the scene from above. I’m a baby and something disturbing, something painful is happening to my body “down there,” and I don’t know what it is. I see a blue cloth and a lot of blood. I see me being passed around by family members, presumably at a table, in a room in a house. I’m swaddled up in a blanket and I’m screaming my lungs out and they are saying to each other, he’s just cranky. The same things always happened in the dream.
I don’t know what this means. I find it hard to believe I can remember something that’s impossible to remember, but having that dream over and over when I was little seems significant. I do know the dreams stopped after I figured out what had happened to me.
I didn’t know what circumcision was until I was 13 or 14, when I saw the word in the Bible that my parents had given me. I looked it up in the dictionary because I’ve always been bookish. I told my parents, “Please not to do this to me,” and their answer was something like, “Well, don’t worry, we already did,” followed by a blind parroting of the same shallow arguments of hygiene and tradition that my frantic and terrified reading through medical almanacs and Bible footnotes had yielded. Dad got angry shortly after he realized I wouldn’t back down. Mom sat in front of the computer searching for a web page that would prove her right with little original thought on her part.
I have my own theories about why my family always joked about it and got defensive when I objected. Everybody deals with pain in their own way. For me, the pain of circumcision and then being ridiculed in my own family for speaking up has shaped my life in profound ways. I’m 30 now. For years I had pickled my thoughts and feelings with alcohol and drugs (mostly alcohol) so I didn’t have to think about that part of my body. If that thing hadn’t happened to me, hadn’t been done to me, I might have been able to stay away from it.
I sought out therapists and told them my struggles stem from circumcision trauma, and they just wrote it off. “Deep down, you’re hurt by something else,” “You can’t be that upset about a piece of skin,” “Don’t you understand they just wanted to help you?” Always being met with resistance by people you trust, starting with your parents and just going forward—that does something to you. It makes you doubt yourself. How could I be wrong for wanting to keep my body the way it was designed? How does someone inflict such harm and horror on their child, and claim it to be an act of love?
Luckily, I’m surrounded by so many friends who are also against cutting baby boys. We’re a very close-knit group. I don’t talk about my feelings or experiences with most of them, but we have a mutual understanding that circumcision is wrong. I was happy when a friend who recently had a baby boy kept him intact.
I want that for every boy. No one should grow up thinking that they’re somebody’s property, or that their wishes for their body don’t matter. Think about it: If boys don’t understand that, when they start dating, they’re not going to understand consent, and a lot of bad is going to happen out of that. Teaching our boys consent starts with protecting their rights to their body.
In our family, I was told there was something wrong with me for wanting to be left whole and being outspoken about it. I was supposed to stay in line and be OK with being cut. But harm is harm, no matter what twisted motivation is used to justify it. People need to remember that whatever they do to a child, they’re not the one who has to live with that. The child is, and they’re going to be an adult one day…still having to live with someone else’s decision.
— Kay Zugar
Interested in lending your voice? Send us an email, giving us a brief summary of what you would like to write about, and we will get back to you.
Dec 4, 2022
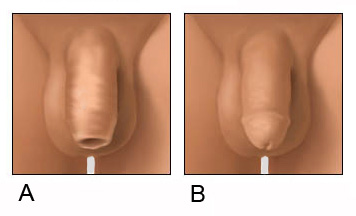
Two recent surveys by Intact America have raised the question by some participants of why we asked the men if their penis looked like A (an intact penis) or B (a circumcised penis), which they found either distasteful or an invasion of privacy. This is the A or B image they were talking about.
The short answer is accuracy. Asking this question improves the quality of the survey results. A lot. The reason is that many men don’t know their penile status! A 2004 study of college-aged men found that 33% were mistaken or unsure of their penile status.[i] This is nothing new, a 1960 study found 14% of men were unsure; their status was confirmed by a physical examination.[ii]
More recently, in Intact America’s three, national random sample surveys (2017, 2018, & 2021) of 3298 Americans, 14% of men were mistaken or unsure of their penile status. See below for my decade-old methodology to determine whether men were mistaken or not. But first, here’s an entertaining anecdote to illustrate the problem.
You may have seen the episode of the Graham Norton Show on BBC in 2017 with guest actor Sir Patrick Stewart. He relayed the funny story about him mentioning in passing to his wife that he was circumcised. According to Stuart, in his 70s at the time, the conversation went something like this:
Stewart: I’m circumcised.
Wife: (laughs) You’re not circumcised.
Stewart: That’s ridiculous! I should know if I’m circumcised! End of conversation.
Stewart: The next day, I happened to be seeing my doctor for my annual physical. When the doc was ‘down there,’ I mentioned my disagreement with my wife, and asked, “I’m circumcised, right?”
Doctor: Not!
Surprisingly, even men who call themselves intactivists, and who are presumably knowledgeable about circumcision and male sexual anatomy, aren’t sure. A survey of intactivists found that 13% of intactivist men are mistaken or unsure.
In 2011, I wanted to learn if newborn circumcision was associated with alexithymia. Alexithymia is the inability to identify and express emotions. It is thought that it is acquired at a very early age. Such people have difficulty in relationships, social interactions, and even in therapy. But I could not examine these men who live across the United States. So, I had to develop a viable validation alternative for that peer-reviewed alexithymia and circumcision study. My solution was to ask their penile status and then compare that with their answer to the A-B image question. Entries that did not match correctly were removed from the dataset.
As it turns out, and unknown to me at the time, I’m not the first researcher to realize that self-report is inaccurate when it comes to penises. In 1992, Schlossberger found that: “Use of visual aids to report circumcision status was more accurate (92%) than self-report (68%).[iii] Wow.
Granted, the best way to determine penile status would be a physical examination. But this is so problematic on so many levels that it would be all but impossible to survey. You’d have to pass certain standards using human subjects, hire medical staff, obtain liability insurance, and of course get permission from the men to disrobe. (By the way, the proper way to determine if a man is circumcised isn’t to look for the lack of a foreskin, but the presence of a circumcision scar.)
The solution that I came up with, and one I’ve used many times since, is a three-part survey-question method. The questioning goes something like this:
Are you circumcised or intact (not circumcised)?
Circumcised
Intact
Don’t know
Which one of these images most looks like your flaccid (not erect) penis?
A
B
Unsure
Are you restoring your foreskin?
Yes
No
I don’t know what this is
As you can see, this method results in much more accurate answers, and provides trustworthy data. Nevertheless, some men are not comfortable answering these questions, even to an anonymous researcher. I can appreciate that. That’s why I’ve taken steps to avoid their discomfort: 1) I inform participants that they’ll be asked personal, sexual questions, 2) tell them they can opt out now, 3) tell them they can opt out at any time, 4) mention that this data will only be used in aggregate form, and that at no time will their identity be revealed, and 5) use the image shown above obtained from a medical illustration stock image source instead of using a photo of real penises.
A study I recently conducted, and now in-press, titled “Adverse Childhood Experiences, Dysfunctional Households, and Circumcision,” also employed this method. None of the journal reviewers mentioned a problem with using this image.
So, not using this tripartite image question would make the results skewed, if not unusable, and therefore unpublishable.
Sadly, many circumcision studies being published since I created this method continue to just ask the men if they are circumcised or not, leaving us unsure of what to make of their conclusions. As scientists like to say: “Junk in, junk out.” (no pun intended!)
—Dan Bollinger
[i] Risser JMH, Risser WL, Eissa MA, Cromwell PF, Barratt MS, Bortot A. Self-assessment of circumcision status by adolescents. Am J Epidemiol. 2004;159:1095–1097.
[ii] Wynder EL, Licklider, SD. The question of circumcision. Cancer. 1960;13(3):442 5. 14.
[iii] Schlossberger N, Turne R & Irwin C (1992) Early adolescent knowledge and attitudes about circumcision: methods and implications for research. J Adolesc Health 13(4): 293-297.
Aug 22, 2022
 Dear Marilyn:
Dear Marilyn:
I’m looking forward to attending Intact 2022, the 16th International Symposium on Child Genital Cutting, in Atlanta this week. Can you tell me how child genital cutting symposia have impacted intactivism since you began organizing them in 1989?
—Larry, St. Louis, MO
Dear Larry:
I first witnessed a circumcision in 1979. I was horrified and immediately began researching the subject. Our local libraries, including those at the hospital and universities, had little or no relevant information. Then in 1980, Edward Wallerstein sent me a copy of his book, “Circumcision: An American Health Fallacy.” This book became the foundation of my work. I told everyone what I was learning and appeared on local radio and television shows. I was contacted by an attorney who wanted to file a lawsuit asking if parents have a right to consent to a child’s circumcision, or if the baby’s body belonged to the baby. I found a plaintiff, and our lawsuit got publicity.
The publicity likely prompted a couple of local doctors—urologist Aaron Fink and Edgar Schoen, a pediatrician—to join forces and begin their campaign to validate both cultural and religious circumcision, in the form of a pro-circumcision resolution that Fink introduced to the California Medical Association (CMA) and Schoen took to the American Academy of Pediatrics (AAP).
Fink introduced his resolution to the CMA at its yearly convention in 1987, but the Scientific Committee voted it down. Fink came back in 1988 with Arthur Dick, a urologist, who circumcised a banana in front of the CMA membership, and the resolution passed. This was followed by a counter-resolution from Dr. John Hardebeck, who planned to present it at the CMA convention the following year. I knew that meeting was being held at the Disneyland Hotel. So I booked a hotel across the street for our First International Symposium on Circumcision.
I invited Dr. Michel Odent, a French obstetrician and childbirth specialist, to give the keynote presentation. He asked if there would be other international presenters and, when I told him I didn’t have any, he said, “Well then, you need me.” I invited Fink and Schoen, but neither came or even responded to my invitation. But those who did were eager to share their work or their experiences. This was the first time that experts from various disciplines—religion, anthropology, psychology, medicine, law, and ethics—gathered around the subject of circumcision. We were all thrilled by what had transpired. Dr. Paul Fleiss, a popular Los Angeles pediatrician who was both a breastfeeding and anti-circumcision advocate, also attended, and—at the end of the symposium—declared: “Marilyn, now we need to take this show on the road.”
The second symposium was held in 1991 in San Francisco, and Dr. Ashley Montagu, anthropologist and humanist, gave the keynote address. Presenters and attendees alike were amazed at the quality, breadth, and depth of the presentations on this crucial human rights issue.
The joy of each symposium is the new material that has been presented, the medical research that has been done, and the focus on how we treat children at the beginning of life and how this affects society. Those who have attended our symposia have been enriched with important information about the issue and what’s being done to end an anachronistic blood ritual. By coming together, we learn from one another, and become secure in knowing we’re not alone. We have become Intactivists together and we have become a family.
In the following years, we held 13 more symposia around the world including Switzerland, England, Australia, Italy, and Finland; six books of the proceedings were published by Springer—the same company that published Wallerstein’s groundbreaking book decades earlier. Our books are now in universities worldwide and being used in classrooms.
The Atlanta symposium (August 2022) will be the first I will not attend in person. While I’m sorry for that, that’s life! And I’m thrilled to know these gatherings will continue—this time because of David Llewellyn and Georganne Chapin—as will the movement I initiated all those years ago just because I couldn’t keep my mouth shut. As you can see, I still can’t. Please, carry on…
—Marilyn Milos, RN
Jul 21, 2022
Since Intact America’s founding in 2008, our organization’s stated goal has been to “change the way America thinks about circumcision.”
Our Vision statement says:
Intact America envisions a world where children are free
from medically unnecessary surgeries carried out on them without their consent
in the name of culture, religion, profit, parental preference, or false benefit.
The genital cutting of any child in the absence of life-threatening or seriously health-threatening pathology violates not only that child’s body, but also his/her/their autonomy over their own sexual future. This position is immutable. No parent or guardian has the right to waive a child’s right to be protected from any type of tortious interference, or physical or sexual assault, with regard to genital cutting. The right that governs is that of the child.
Intact America was founded in 2008 by a coalition of individuals and intactivist organizations who wished to see the intactivist movement grow into a mainstream human rights cause. The new organization, as well as its founders, were guided by widely-accepted secular bioethical principles adopted in Western human rights and political discourse in response to atrocities committed against persons of many religions, races, and cultures during World War II. Our position is also supported by common law and the objective fact that having normal genitals, including a foreskin, is not a condition requiring surgical intervention. Furthermore, intactivism places no inherent value in following a particular common or traditional practice nor in capitulating to the current (but always-evolving) status quo, if those traditions and practices compromise the physical integrity and sexual wellbeing of children and the adults they will become.
Thus, neither religion nor “culture” should ever be invoked to support child genital cutting. At the same time, opposition to child genital cutting is not rooted in anti-religious sentiments. To tie ourselves up in such accusations is to lose focus on the true intent of the intactivist movement, as expressed in the fundamental goal and vision of Intact America, restated from above: a world where children are free from medically unnecessary surgeries carried out on them without their consent.
As a human rights organization that respects all persons regardless of their race, religious or cultural affiliation, it is also our duty to refute expressions of bigotry when expressed by people outside or within the intactivist movement. To leave no doubt, in 2022 Intact America’s adopted a new position statement against bigotry and hate speech:
Intact America rejects all forms of ethnic, racial, and religious stereotypes and bigotry. We condemn any form of hate speech based on ethnicity, race, national origin, gender, sexual orientation, religion, or irreligion. The incorporation of anti-Semitic or anti-Muslim expressions into criticism of male (or female) circumcision only serves to undermine our movement and potentially derail our work to protect all children from genital cutting.
I fervently believe that adherence to the logic and principles outlined above will ensure our success in protecting future children and the adults they will become.
–Georganne Chapin
Dec 1, 2021
On October 11, 2021, the New Yorker magazine published an essay by popular writer Gary Shteyngart, recounting how being circumcised when he was seven years old resulted in decades of misery and complications. On November 1, the magazine published three comments in response, mine, one from a rabbi, and one from a urologist. The post below is the follow-up letter I wrote to the urologist, Dr. Michael Mooreville.
Dear Dr. Mooreville:
I am writing about your letter to the New Yorker, which appeared after my own among the responses to Gary Shteyngart’s essay about his decades of suffering because of a botched circumcision. Thank you, in advance, for taking the time to read my comments below.
First, you suggest that Shteyngart’s problems occurred because he was circumcised too late, and then say that it’s easier (somehow) for a physician to know how much foreskin to remove from a baby than from an older male. My decades of working to end unconsented-to, medically unnecessary circumcision suggest this is not true. Men who have spoken or written to me, or who have spoken out publicly about their circumcision-induced penile deformities, overwhelmingly were circumcised as newborns by doctors in American hospitals. Some of them have undergone one or more additional surgeries to correct cosmetic or functional problems; others, out of parental ignorance or shame, instead have learned to live with the harm just as Shteyngart did. In none of these cases did any of these surgeries result in a better, healthier penis than the penises of men who were fortunate enough to have grown up with their natural, unaltered genitalia. As a practicing American urologist, your caseload is likely similar to that of other urologists who have told me that more than one-quarter of their medical practice involves addressing circumcision-related damage, including meatal stenosis (which occurs nearly exclusively in circumcised males), skin bridges (such as Shteyngart’s), and degloved penile shafts.
Second, I am curious about your comment that amputating a baby’s foreskin will allow his penis to “grow into a fully mature look…” (emphasis mine). Are you suggesting that the penises of men with foreskins (comprising around 75% of the world’s males) are somehow “immature”; this makes no sense. How can a penis shorn of its natural protective covering, with its nerves, muscles and blood supply be superior to the natural, unaltered penis that evolved over hundreds of thousands of years? Frankly, I’m astonished that the New Yorker’s rigorous fact-checking protocol didn’t eliminate this nonsensical statement from your letter.
Finally, I wonder if there are other healthy body parts you would suggest removing from babies or children because they “can be the source of multiple (?) medical problems in older men” (or women). The appendix (1.1 cases of appendicitis per 1000)? Teeth (prone to infection-causing decay)? Breasts (1 case per 1000 of breast cancer among American women aged 40, increasing over time), while the rate of penile cancer (which occurs in both intact and circumcised men) in the United States is 1 per 100,000. I might add here that genital hygiene is not complicated. If a boy can learn to become a teacher or chef or woodworker or tennis player or truck driver or urologist, he should be able to learn how to wash his penis.
I hope you will think about my questions, and dare to think in a more common-sense way about a forced bodily alteration that does nothing to make American boys or men healthier than their counterparts in countries where males retain the genitals they are born with.
Sincerely,
Georganne Chapin, MPhil, JD
Executive Director